


 In 2025, NIH Pragmatic Trials Collaboratory investigators published new study designs and trial results, shared insights from program leadership, and developed innovative methods in the design, conduct, implementation, and dissemination of pragmatic clinical trials. Their work included perspectives from the Coordinating Center, best practices from the Core Working Groups, and results from the NIH Collaboratory Trials.
In 2025, NIH Pragmatic Trials Collaboratory investigators published new study designs and trial results, shared insights from program leadership, and developed innovative methods in the design, conduct, implementation, and dissemination of pragmatic clinical trials. Their work included perspectives from the Coordinating Center, best practices from the Core Working Groups, and results from the NIH Collaboratory Trials.
The program contributed 45 articles to the peer-reviewed literature this year, including the primary results of the ACP PEACE, BackInAction, HiLo, INSPIRE, and PRIM‑ER trials. Cross-Core and cross-Trial collaborations led to the sharing of important lessons from the conduct of multiple NIH Collaboratory Trials.
The total number of published articles from the program reached 386.
Coordinating Center
- Ensuring virtual vigilance in decentralized clinical trials
- Intervention delivery complexity and adaptations for implementation of non-pharmacologic pain interventions
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
Cross-Core and Cross-Trial Collaborations
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- Collection of patient-reported outcome measures in rural and underserved populations
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
Distributed Research Network
Core Working Groups
Biostatistics and Study Design Core
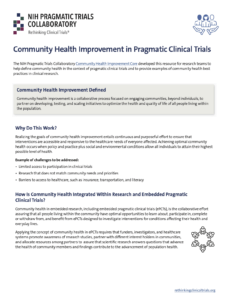
Community Health Improvement Core
Electronic Health Records Core
Ethics and Regulatory Core
- Untapped potential? Representativeness in pragmatic trials
- Ethical considerations for sharing aggregate results from pragmatic clinical trials
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
- Disentangling informing participants from obtaining their consent
- Empirical research related to the ethics of pragmatic clinical trials: A scoping review
- Reflections on a principal of research ethics: Tom Beauchamp, moral specification, and waivers of informed consent
Health Care Systems Interactions Core
Patient-Centered Outcomes Core
NIH Collaboratory Trials
ABATE Infection
ACP PEACE
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
- [Main outcomes] An intervention to increase advance care planning among older adults with advanced cancer: A randomized clinical trial
ARBOR-Telehealth
BackInAction
- Recruitment and retention for an acupuncture trial in an underrepresented 65 and older population with chronic low back pain
- Baseline sample characteristics for the BackInAction pragmatic trial of acupuncture for chronic low back pain in older adults
- [Main outcomes] Acupuncture for chronic low back pain in older adults: A randomized clinical trial
- Cost-effectiveness of acupuncture needling for older adults with chronic low back pain
BeatPain Utah
BEST-ICU
EMBED
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
FM-TIPS
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- Collection of patient-reported outcome measures in rural and underserved populations
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
- Building community through data: The value of a researcher driven open science ecosystem
- Community engagement strategies improve rural enrollment in a pragmatic clinical trial
GGC4H
GRACE
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- A scoping review of social determinants of health and pain outcomes in sickle cell disease
- Collection of patient-reported outcome measures in rural and underserved populations
HiLo
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
- [Main outcomes] Higher versus lower phosphate targets for patients undergoing incenter hemodialysis: A randomized controlled trial
I CAN DO Surgical ACP
IMPACt-LBP
INSPIRE
- [Main outcomes] Improving empiric antibiotic selection for patients hospitalized with skin and soft tissue infection: The INSPIRE 3 Skin and Soft Tissue randomized clinical trial
- [Main outcomes] Improving empiric antibiotic selection for patients hospitalized with abdominal infection: The INSPIRE 4 cluster randomized clinical trial
- Initial antibiotic selection strategy and subsequent antibiotic use: Insights from the INSPIRE trials
iPATH
LIRE
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
MOMs Chat & Care Study
NOHARM
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- Collection of patient-reported outcome measures in rural and underserved populations
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
- Evaluating physical and occupational therapists' experiences implementing an electronic health record-based intervention to support perioperative patients’ use of nonpharmacological pain management techniques
- Delivering an electronic health record based educational intervention promoting peri-operative non-pharmacological pain care as part of a randomized controlled trial: Mixed method evaluation of inpatient nurses' perspectives
- Patients' peri-operative experiences with non-pharmacologic pain care techniques: A secondary qualitative analysis of the NOHARM trial
Nudge
OPTIMUM
- Collection of patient-reported outcome measures in rural and underserved populations
- The hidden complexity of conducting mindfulness-based group medical visits: Comfort, challenge, and the influence of social determinants of health
- Increasing equity within randomized control trials: A qualitative analysis of focus groups from a multi-site, pragmatic clinical trial
- Prevalence of chronic overlapping pain conditions in participants with chronic low back pain enrolled in a pragmatic trial of mindfulnessbased stress reduction
PRIM-ER
- [Main outcomes] Palliative care initiated in the emergency department: A cluster randomized clinical trial
- Palliative care in the emergency department—Reply
- Bayesian hierarchical penalized spline models for immediate and time-varying intervention effects in stepped wedge cluster randomized trials
- Acute care use and prognosis in older adults presenting to the emergency department
- Healthy days at home and prognosis of older adults with cancer and non-cancer serious life-limiting illnesses
- Effect of a multi-component palliative care intervention on goals of care discussions for critical patients in the emergency department
SPOT
- Impact of electronic health record updates and changes on the delivery and monitoring of interventions in embedded pragmatic clinical trials
- Monitoring in pragmatic trials: Lessons from the NIH Pragmatic Trials Collaboratory
 The NIH Pragmatic Trials Collaboratory’s
The NIH Pragmatic Trials Collaboratory’s  The NIH Pragmatic Trials Collaboratory has launched a new learning module,
The NIH Pragmatic Trials Collaboratory has launched a new learning module,  Pragmatic clinical trials embedded in healthcare systems rely on partnerships between investigators and healthcare system leaders to conduct research. As the end of a pragmatic trial approaches, research teams and their partners often face uncertainties around this undefined phase when researchers are waiting on results. End-of-trial decision-making, including whether to sustain an intervention, has implications for research teams, healthcare systems, and patients.
Pragmatic clinical trials embedded in healthcare systems rely on partnerships between investigators and healthcare system leaders to conduct research. As the end of a pragmatic trial approaches, research teams and their partners often face uncertainties around this undefined phase when researchers are waiting on results. End-of-trial decision-making, including whether to sustain an intervention, has implications for research teams, healthcare systems, and patients. In an article
In an article  In a JAMA Viewpoint published online this week, leaders from the NIH Pragmatic Trials Collaboratory discuss the discordance between the results of pragmatic clinical trials and the implementation of those results in healthcare settings, even in settings that championed the work.
In a JAMA Viewpoint published online this week, leaders from the NIH Pragmatic Trials Collaboratory discuss the discordance between the results of pragmatic clinical trials and the implementation of those results in healthcare settings, even in settings that championed the work.