In a new NIH Collaboratory study, 20 NIH Collaboratory Trials responded to a survey about challenges encountered when using the electronic health record (EHR) for pragmatic clinical research. The goal of the study was to elucidate challenges and develop solutions—or prerequisites for pragmatic research—to enable healthcare system leaders, policy makers, and EHR designers to improve the national capacity for generating real-world evidence.
The article was published in the Journal of American Medical Informatics Association (JAMIA).
The challenges identified by the projects fell into 6 broad themes, including inadequate collection of patient-centered data, lack of functionality for structured data collection, lack of standardization, lack of resources to support customization, difficulties aggregating data from multiple sites, and difficult and inefficient access to EHR data.
Researchers from the NIH Collaboratory’s EHR Core and colleagues from the Patient-Centered Outcomes and the Health Care Systems Interactions Core Working Groups discussed the issues and iterated possible solutions. The authors developed the following prerequisites for the conduct of pragmatic research:
Integrate collection of patient-centered data into EHR systems
Facilitate structured research data collection by leveraging standard EHR functions, usable interfaces, and standard workflows
Support creation of high-quality research data by using standards
Ensure adequate IT staff to support embedded research
Create aggregate, multidata type resources for multisite trials
Create reusable and automated queries
The authors argue for the ability to tailor EHR systems to enable the collection of patient-centered outcomes and the extraction of high-quality, standardized data. Although the primary uses of the data are for clinical care and billing, high-quality data from the EHR also have the potential to improve clinical care and population health by providing reliable evidence and to support pragmatic research and learning within and across healthcare systems.
This work was supported within the National Institutes of Health (NIH) Health Care Systems Research Collaboratory by the NIH Common Fund through cooperative agreement U24AT009676 from the Office of Strategic Coordination within the Office of the NIH Director. This work was also supported by the NIH through the NIH HEAL Initiative under award number U24AT010961.
Leaders of the NIH Collaboratory’s Health Care Systems Interactions Core Working Group spoke in a recent interview about the impacts of the COVID-19 pandemic on the NIH Collaboratory Trials.
“Some of the projects are facing healthcare systems that are on pause for research,” said Leah Tuzzio, a senior research associate at Kaiser Permanente Washington Health Research Institute (KPWHRI) and a member of the Core. “It’s happened before when policy changes or when [electronic health record] systems change or when someone important leaves, but the pandemic has had a huge impact,” she said.
“Healthcare systems are strongly influenced by the environment and by changes in their environment, and so any pragmatic trial that’s really embedded in the healthcare system will be affected by the environment around it,” said Dr. Eric Larson, a KPWHRI senior investigator and the chair of the Core. Healthcare systems participating in the NIH Collaboratory NIH Collaboratory Trials have been overwhelmed by their number one priority, which—in addition to caring for their patients—is adapting to COVID, Larson said.
In addition to guiding the NIH Collaboratory Trials through pandemic-related challenges, the Health Care Systems Interactions Core has been working on several long-term projects.
“One of the things that we’re currently working on is a typology of the healthcare systems that have participated in [the GRACE and BeatPain Utah NIH Collaboratory Trials] as well as the projects that came before,” said Core project manager Rachel Hays. The Core is surveying NIH Collaboratory Trial investigators about what lessons they would pass on to future pragmatic trial investigators about building partnerships with their participating healthcare systems, she said.
Survivor Corps is an online community of 170,000 patients affected by COVID-19 and their families and friends. The advocacy group is using its members’ collective experience to build a repository of data sets and research tools to support COVID-19 research, including studies of post-COVID conditions, or “long COVID.” The group seeks to fill the gap between real-world evidence and scientific research to advance understanding of the disease and patients’ healthcare options.
“We have been sort of the canary in the COVID coal mine from the beginning,” said Berrent, who founded Survivor Corps in March 2020 after becoming one of the first people in the United States to be diagnosed with COVID-19.
Berrent will be joined during Grand Rounds by Survivor Corps research director Dr. Natalie Lambert and by Nick Guthe, a Survivor Corps member and adviser.
Survivor Corps’s website, which has been selected by the US Library of Congress for inclusion in the nation’s Coronavirus Web Archive, serves as a hub to provide support, information, and education about COVID-19, connect patients to researchers, and facilitate the nation’s COVID-19 response.
The NIH Collaboratory Coordinating Center is using its popular Grand Rounds platform to share late-breaking research and promote resources in support of clinical researchers affected by the COVID-19 public health emergency. For previous COVID-19 Grand Rounds, and more news and resources related to the COVID-19 public health emergency, see the COVID-19 Resources page.
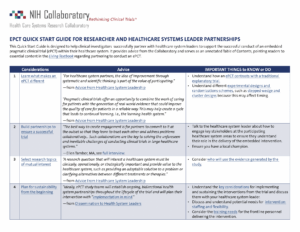
The NIH Collaboratory is pleased to share a new resource to help clinical investigators successfully partner with healthcare system leaders. The Quick Start Guide for Researcher and Healthcare Systems Leader Partnerships provides advice from NIH Collaboratory and healthcare system leadership and serves as an annotated table of contents for the Living Textbook, pointing readers to essential content.
The Quick Start Guide is part of a series of tools intended to support the successful conduct of ePCTs within healthcare systems. The first guide in the series, the Quick Start Guide for Investigators, is designed for clinical investigators interested in learning how to conduct an ePCT. The NIH Collaboratory Coordinating Center is developing more Quick Start Guides for different audiences and use cases.
In an article published today in the New England Journal of Medicine, Drs. Richard Platt, Adrian Hernandez, and Greg Simon of the NIH Collaboratory discuss barriers to healthcare system participation in embedded research and strategies for improvement.
“We advocate creating a robust national [embedded pragmatic clinical trial] capability to generate evidence to guide decisions by patients, clinicians, health systems, and regulators and respond to urgent national health crises, like COVID-19 or the opioid crises,” the authors wrote.
The article recommends a 4-pronged strategy that researchers and funders should consider to increase healthcare system participation in pragmatic clinical trials:
Reimburse for the additional costs of trial participation.
In some highly engaged systems, support permanent, reusable infrastructure.
Offload research-specific tasks to minimize burden on sites (such as IRB oversight, obtaining informed consent, and mailing medications to participants).
Assign and promote reputational benefit for these activities.
In a new article in Healthcare’s special issue on embedded research, Leah Tuzzio and colleagues use experiences from the NIH Collaboratory to describe how quality improvement activities may pose challenges for embedded pragmatic clinical trials (ePCTs), especially if there are overlapping goals and timelines.
For ePCTs to be rigorous, study teams must monitor, adapt, and respond to QI during the design and the trial implementation. Both ePCTs and QI happen within the same context and aim to improve patient care, and they are inherently interconnected. — Tuzzio et al, Healthcare, 2021
ePCTs tend to be larger and more broadly generalizable than quality improvement initiatives and may generate high-quality evidence for care and clinical practice guidelines. Quality improvement initiatives may address the same high-impact health questions, but if they co-occur with ePCTs, they may dilute or confound the ability to detect change. As a result, study teams may need to monitor, adapt, and respond to quality improvement initiatives during the design and conduct of the trial. The authors suggest that routine collaboration with healthcare system stakeholders can help align research and quality improvement to support high-quality, patient-centered care.
Publication of the special issue was supported by AcademyHealth.
BeatPain Utah Julie Fritz, PhD, PT Associate Dean for Research, College of Health Adjunct Professor, Orthopaedic Surgery Distinguished Professor, Physical Therapy & Athletic Training Adjunct Professor, Orthopaedic Surgery Operations University of Utah
David Wetter, PhD, MS Professor, Population Health Sciences Adjunct Professor, Psychology University of Utah
STOP CRC Gloria Coronado, PhD Distinguished Investigator Mitch Greenlick Endowed Scientist for Health Disparities Kaiser Permanente Center for Health Research
Amanda Petrik, MS Sr. Research Associate Center for Health Research Kaiser Permanente Northwest
Guest Moderator:
Wendy Weber, ND, PhD, MPH Chief, Clinical Research in Complementary and Integrative Health Branch Division of Extramural Research National Center for Complementary and Integrative Health (NCCIH) National Institutes of Health (NIH)
Topic
Inclusion of Diverse Participants in Pragmatic Clinical Trials: Planning for Diversity – Stakeholder Engagement and Site Selection to Maximize Diversity
Keywords
Participant diversity; Stakeholder engagement strategies; STOP CRC; BeatPain Utah; Health equity; Community health centers; Plan-Do-Study-Act
Key Points
Disparities in pain prevalence and pain management are well established. In particular, odds of receiving opioids for pain management are greater, and odds of nonpharmacologic care lower, in rural, low income, and Latinx communities.
It is essential that communities and researchers come together to create long-term solutions to prevent cancer, chronic and infectious disease, and improve health among underserved populations. Research projects should be driven by the priorities of community partners.
Study advisory boards can include health center leaders, patient advocates, legislators, and community organization leaders. These boards provide local context and, in the case of STOP CRC, they identified policy changes that were needed around access to colorectal cancer screening.
Discussion Themes
Sharing information and resources with community partners—and responding to their needs and building their capacity—helps to build trust around medicine and research.
To what extent is it important to show evidence of interest in and respect for the community beyond the specific focus of your initiative? For example, participating in important community activities and developing a deeper understanding of the culture.
We must design and plan for sustainability at the outset, and we must make targeted, specific efforts to ensure the inclusion of diverse populations in clinical trials.
Another way to increase diversity is to prepare and train more scientists and investigators from diverse populations.
The NIA IMPACT Collaboratory has announced 3 new funding opportunities for researchers at all levels who are interested in pragmatic clinical trials embedded in healthcare systems (ePCTs). They include funding for NIH Collaboratory Trials, a new scholars program for junior and senior investigators, and a new cycle of funding for 1-year pilot studies.
NIH Collaboratory Trials Program: The IMPACT Collaboratory will fund up to 2 NIH Collaboratory Trials designed as full-scale ePCTs that test nonpharmacological interventions for people living with Alzheimer disease and related dementias (ADRD) and their care partners. The projects should generate evidence on effective care delivery practices that can be expanded or implemented in other healthcare systems. An informational webinar will be held on Thursday, February 11, at 2:00 pm ET.
Health Care System Scholars Program – A new Health Care Systems Embedded Research Scholars Program offers junior and senior investigators an opportunity to work directly with healthcare systems interested in improving the care provided to people living with dementia and their care partners. A informational webinar will be held on Thursday, February 11, at 1:00 pm ET.
Pilot Grants Program: One-year pilot studies are meant to generate preliminary data necessary to design and conduct future full-scale ePCTs. The IMPACT Collaboratory will consider applications for pilot studies that test nonpharmacological interventions embedded in healthcare system for people living with ADRD and their care partners. An informational webinar will be held on Monday, February 22, at 4:00 pm ET.
The NIA IMPACT Collaboratory is supported by a grant from the National Institute on Aging. Its mission is to advance care for persons with dementia and their caregivers in real-world settings by building national capacity to conduct pragmatic clinical trials that test interventions embedded in healthcare systems.
Renato D. Lopes, MD, MHS, PhD Professor of Medicine Division of Cardiology Duke University Medical Center Duke Clinical Research Institute Brazilian Clinical Research Institute
Topic
Generating High-Quality Evidence During a Pandemic: The Brazilian COALITION Experience
The SARS-CoV-2 infection affects the cardiovascular system and is associated with complications such as myocardial ischemia, myocarditis, arrhythmias, and thromboembolic events. These manifestations result mainly from the intense systemic inflammatory response and disorders of the coagulation system.
The COALITION collaborative includes several major Brazilian hospitals and research networks with the aim of accelerating multicenter randomized controlled trials that generate high-quality evidence to guide the treatment of patients with COVID-19.
To move toward a world in which most clinical decisions are supported by high-quality evidence requires structural changes in the clinical trials ecosystem.
Discussion Themes
How did you overcome contractual and regulatory concerns to execute your trials?
Instead of “publish or perish,” it should be “collaborate or perish.” Collaboration is the key to surviving in modern academic medicine.
Read more about the need for high-quality evidence to treat COVID-19 patients in Anticoagulation in COVID-19: It Is Time for High-Quality Evidence (J Am Coll Cardiol, 2020)