Even in minimal-risk studies that do not use the standard consent process, there may be value in informing participants about the research. Such notifications should be considered the default for clinical trials conducted under a waiver of informed consent, argue the authors of a new report from the NIH Pragmatic Trials Collaboratory.
Pragmatic clinical trials conducted in the context of routine healthcare often meet the regulatory criteria for a waiver or alteration of the standard informed consent process. In such cases, researchers and reviewers might assume there is no reason to communicate information about the study to participants. However, providing information to participants, even in minimal-risk research conducted with a waiver of consent, can promote important ethical values.
Experts from the NIH Collaboratory’s Ethics and Regulatory Core teamed up with investigators from several of the NIH Collaboratory Trials to describe methods of informing participants in minimal-risk research.
The investigators used a variety of notification approaches in their studies, including letters and email campaigns, posters in waiting rooms and other common areas, conversations with clinicians, and presentations at staff meetings. The amount of information provided to participants ranged from a general statement that research was being conducted at the institution to detailed information about the study in question.
“When a study is approved with a waiver of research consent, investigators and review committees should consider on a case-by-case basis what information, if any, to disclose to participants, and how it will be disclosed,” the authors wrote. The costs, benefits, and feasibility of these approaches vary from study to study.
Communicating information to participants can promote several important goals:
The ethical principle of respect for persons
Participants’ understanding of the study and of research in general
Participants’ understanding of their contributions to the research
Participants’ ability to voice and discuss any concerns about the study
Participant engagement in research
Trust in research and researchers
“Providing information to the participants should thus be the default for trials conducted under a waiver of research consent,” the authors wrote.
In 2012, the NIH Common Fund established the NIH Health Care Systems Research Collaboratory. The goal of the program is to improve the way clinical trials are conducted by creating an infrastructure for collaborative research with healthcare systems. The NIH Collaboratory launched with a Coordinating Center, Core Working Groups, and NIH Collaboratory Trials to conduct embedded pragmatic clinical trials (ePCTs) in partnership with healthcare system leaders and to work collaboratively with the NIH to solve problems as they arise, develop best practices, and share lessons and resources to with others conducting ePCTs.
Collaboratory Mission: Strengthen the national capacity to implement cost-effective large-scale research studies that engage healthcare delivery organizations as research partners.
With the first round of NIH Collaboratory Trials nearing completion, the project teams are beginning to publish results and share lessons with other researchers. We asked the principal investigators of the most recently completed projects to share insights about the important contributions of their studies.
Congratulations on finishing your NIH Collaboratory Trial: What do you think is the most important contribution of your study?
ABATE was conducted to determine whether routine bathing and showering with chlorhexidine soap would reduce multidrug-resistant organisms and bloodstream infections compared with usual care. The trial was conducted in 53 HCA Healthcare hospitals (194 non–critical care units)and included 340,000 patients in the intervention period.
“We found that there was no overall benefit to universal antiseptic bathing in non–intensive care units (ICUs). This is in stark contrast to the huge benefit demonstrated in ICUs in the REDUCE-MRSA trial, and may reflect the fact that non–critical care patients stay only a few days in the hospital and are less likely to develop infection. Nevertheless, we did find that antiseptic bathing and nasal decolonization reduced bloodstream infections and antibiotic-resistant organisms by over 30% in patients with devices outside of the ICU. This is important because they are 10% of the non-ICU population, but responsible for over half of bloodstream infections. They provide a valuable targeted population who appear to benefit from this intervention.”
LIRE was conducted to test the effectiveness of a simple and inexpensive intervention: inserting epidemiologic benchmarks into lumbar spine imaging reports. The goal of the trial was to reduce subsequent tests and treatments, including cross-sectional imaging (such as magnetic resonance imaging and computed tomography), opioid prescriptions, spinal injections, or surgery.
“I think that one of the most important contributions of the LIRE trial was demonstrating the feasibility of randomizing hundreds of thousands of patients to receive or not receive an intervention that we inserted into the radiology report. Before our trial began, there was a fair amount of skepticism about whether radiologists would accept routinely inserting prevalence information into their reports on a wide scale. We showed without a doubt that it was feasible.”
PPACT was designed to assess the potential benefit of helping patients adopt self-management skills for chronic pain, limit use of opioid medications, and identify factors amenable to treatment in the primary care setting in three Kaiser Permanente (Northwest, Georgia, and Hawaii) involving approximately 800 patients.
“We started a trial when everybody was still uncertain about what the trade-offs between external validity (and real-world issues that are important for implementation) and the rigor of internal validity. I don’t know if we got that right. There was an assumption that the trial needed to be cluster randomized, and I think it’s informative that only 1 of the 11 NIH-DOD-VA Pain Management Collaboratory trials was cluster randomized. We needed to be able to incubate, have embedded teams stay over time, and really shift the culture. Patients needed to get used to the idea of non-pharmacotherapy over several months, and we may have had more success if we had individually randomized our cohort. I learned a lot in this process.”
PROVEN was designed to evaluate the effectiveness of advance care planning video tools in the nursing home setting by partnering with 2 large healthcare systems that operate 492 nursing homes nationwide.
“PROVEN found an ACP Video Program did not significantly impact hospital transfers, burdensome treatments, or hospice enrollment among nursing home residents with advanced illness, however intervention fidelity was low. Nonetheless, PROVEN was one of the first large pragmatic trials conducted in US nursing homes. Thus, I feel its greatest contribution was setting a foundation of knowledge for the field in terms of methodologies that enable pragmatic trials in this setting and challenges to overcome.”
STOP CRC was conducted to determine whether EHR-embedded tools and clinic staff training in how to implement a mailed fecal immunochemical test (FIT) outreach program could increase colorectal cancer screening uptake among patients with historically lower CRC screening rates and worse CRC outcomes, such as those with low income, or who are on Medicaid or underinsured. STOP CRC was conducted in 26 Federally Qualified Health Centers (FQHCs) in Oregon and California and involved approximately 41,000 patients.
“The ability to work with FQHCs and their new electronic data systems was an important contribution. FQHC settings are not organized healthcare systems, such as Kaiser Permanente, where research is more routine. I think we contributed to the success of this type of research and enabled the FHQCs’ ability to do more of it.” — Dr. Beverly Green
“Our study designed real-time electronic health record tools to allow clinics to mail cancer screening tests to adults who were overdue. We learned a lot about the challenges clinics faced in implementing the program. We shared our learnings with hundreds of additional community clinics in Washington, Oregon, California to help them anticipate and overcome these challenges.”— Dr. Gloria Coronado
TiME was conducted to determine whether treatment with hemodialysis sessions that are longer than many patients in the United States currently receive reduces the high rate of mortality among people being treated with thrice-weekly maintenance hemodialysis. The trial was conducted in 2 large US dialysis provider organizations, DaVita, Inc. and Fresenius Medical Care – North America, and included 266 outpatient dialysis facilities with 7035 patients.
“TiME established a model for conducting real-world research for a group of patients for whom there is very little clinical trial data. Many of the approaches and lessons from TiME are now being applied to a new set of pragmatic trials in dialysis that are being conducted in the US and internationally. In my view, TiME’s greatest contribution was to create a foundation for ongoing efficient and rigorous evidence generation in dialysis.”
Data and resources from the NIH Collaboratory Trials are posted on the NIH Collaboratory’s Data and Resource Sharing page in the coming months. As part of the program’s commitment to sharing, all NIH Collaboratory Trials are expected to share data and resources, such as protocols, consent documents, public use datasets, computable phenotypes, and analytic code.
NIH Collaboratory researchers in 2019 continued to generate new knowledge and research methods in pragmatic clinical trials. Their work included insights from the Coordinating Center and Core Working Groups, large-scale analyses of data from the NIH Collaboratory Distributed Research Network, and results and innovative methodological approaches from the NIH Collaboratory Trials.
So far this year, the NIH Collaboratory has produced nearly 3 dozen articles in the peer-reviewed literature, including the primary results of the ABATE Infection trial, confirmation by the TiME trial of the feasibility of embedding large pragmatic trials in clinical care, and more:
An integrated web application for decision support and automation of EHR workflow: a case study of current challenges to standards-based messaging and scalability from the EMBED trial. JAMIA Open. 2019 Oct 14. [Epub ahead of print]
Although maintenance hemodialysis has long been a staple of care for patients with end-stage renal disease, there are limited data from clinical trials to inform optimal approaches, including the optimal duration of hemodialysis sessions. The TiME trial investigators, in partnership with 2 large dialysis provider organizations, evaluated the effects of a longer hemodialysis session duration on mortality and hospitalization rate among more than 7000 patients receiving care in 266 dialysis facilities.
The TiME trial was discontinued early (median follow-up, 1.1 years) because there was an insufficient difference in mean hemodialysis session duration between the intervention group and the usual care group. The investigators observed no reduction in mortality or hospitalization rate in either group.
Despite ending early, the trial met important objectives for informing the implementation of large pragmatic clinical trials embedded in health care systems. In a large multicenter study with no onsite research personnel, the investigators quickly and efficiently enrolled a large number of participants using an opt-out consent approach. The study data were obtained entirely from the electronic health and administrative records of the partnering dialysis provider organizations and were generated from routine clinical care delivery.
“The TiME trial provides an important foundation for future pragmatic trials in dialysis as well as in other settings,” said Dr. Laura M. Dember of the University of Pennsylvania Perelman School of Medicine, the principal investigator of the TiME trial.
The TiME trial was supported within the NIH Collaboratory by a cooperative agreement from the National Institute of Diabetes and Digestive and Kidney Diseases and received logistical and technical support from the NIH Collaboratory Coordinating Center. Download a study snapshot about the TiME trial, and learn more about the NIH Collaboratory Trials.
A new article published in the journal Trials provides a look at how the Pragmatic–Explanatory Continuum Indicator Summary, or PRECIS, rating system can be applied to clinical trials designs in order to examine where a given study sits on the spectrum of explanatory versus pragmatic clinical trials.
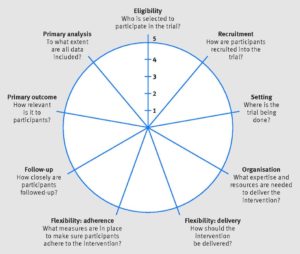
The PRECIS-2 criteria are used to rate study designs as more or less “pragmatic” according to multiple domains that include participant eligibility, recruitment methods, setting, organization, analysis methods, primary outcomes, and more. In this context, “pragmatic” refers to trials that are designed to study a therapy or intervention in a “real world” setting similar or identical to the one in which the therapy will actually be used. Pragmatic trials stand in contrast to explanatory trials, which are typically designed to demonstrate the safety and efficacy of an intervention under highly controlled conditions and in carefully selected groups of participants, but which may also be difficult to generalize to larger or more varied populations.
PRECIS-2 Wheel. Kirsty Loudon et al. BMJ 2015;350:bmj.h2147. Copyright 2015 by British Medical Journal Publishing Group. Used by permission.
Clinical trials are almost never wholly “explanatory” or wholly “pragmatic.” Instead, many studies exist somewhere on a spectrum between these two categories. However, understanding how these different attributes apply to trials can help researchers design studies that are optimally fit for purpose, whether that purpose is to describe a biological mechanism (as in an explanatory trial) or to show how effective an intervention is when used across a broad population of patients (as in a pragmatic trial).
In their article in Trials, authors Karin Johnson, Gila Neta, and colleagues applied PRECIS-2 criteria to 5 pragmatic clinical trials (PCTs) being conducted through the NIH Collaboratory. Each trial was found to rate as “highly pragmatic” across the multiple PRECIS-2 domains, highlighting the tool’s potential usefulness in guiding decisions about study design, but also revealing a number of challenges in applying it and interpreting the results.
Study authors Johnson and Neta will be discussing their findings during the NIH Collaboratory’s Grand Rounds on Friday, January 22, 2016 (an archived version of the presentation will be available the following week).
Johnson KE, Neta G, Dember LM, Coronado GD, Suls J, Chambers DA, Rundell S, Smith DH, Liu B, Taplin S, Stoney CM, Farrell MM, Glasgow RE. Use of PRECIS ratings in the National Institutes of Health (NIH) Health Care Systems Research Collaboratory. Trials. 2016;17(1):32. doi: 10.1186/s13063-016-1158-y. PMID: 26772801. PMCID: PMC4715340.
You can read more about the NIH Collaboratory PCTs featured as part of this project at the following links:ABATE (Active Bathing to Eliminate Infection)
LIRE (A pragmatic trial of Lumbar Image Reporting with Epidemiology)
PPACT (Collaborative Care for Chronic Pain in Primary Care)
STOP-CRC (Strategies & Opportunities to Stop Colon Cancer in Priority Populations)
TIME (Time to Reduce Mortality in End-Stage Renal Disease)
Additional Resources
An introductory slide set on PCTs (by study author Karin Johnson) is available from the Living Textbook:
Introduction to Pragmatic Clinical Trials
The University of Colorado Denver - Anschutz Medical Campus publishes an electronic textbook on pragmatic trials:
Pragmatic Trials: A workshop Handbook



 Even in minimal-risk studies that do not use the standard consent process, there may be value in informing participants about the research. Such notifications should be considered the default for clinical trials conducted under a waiver of informed consent, argue the authors of a new report from the NIH Pragmatic Trials Collaboratory.
Even in minimal-risk studies that do not use the standard consent process, there may be value in informing participants about the research. Such notifications should be considered the default for clinical trials conducted under a waiver of informed consent, argue the authors of a new report from the NIH Pragmatic Trials Collaboratory.