


What is a Pragmatic Clinical Trial?
Section 5
PRECIS-2 Case Study
Focusing on the trial’s intention is the first step in designing a trial that successfully answers its primary research question. For an introduction, read Promoting Both Internal and External Validity: Designing the Trial to Match Its Intention, which describes considerations for choosing a pragmatic or explanatory approach. While both approaches are valuable, their purposes are different and will lead to different design choices. As a result, designs that are more pragmatic will have conclusions and recommendations that are more useful for clinical or policy decision-making, and designs that are more explanatory will be more helpful in expanding scientific knowledge.
Case Study of Trial Design in a Renal Dialysis Setting
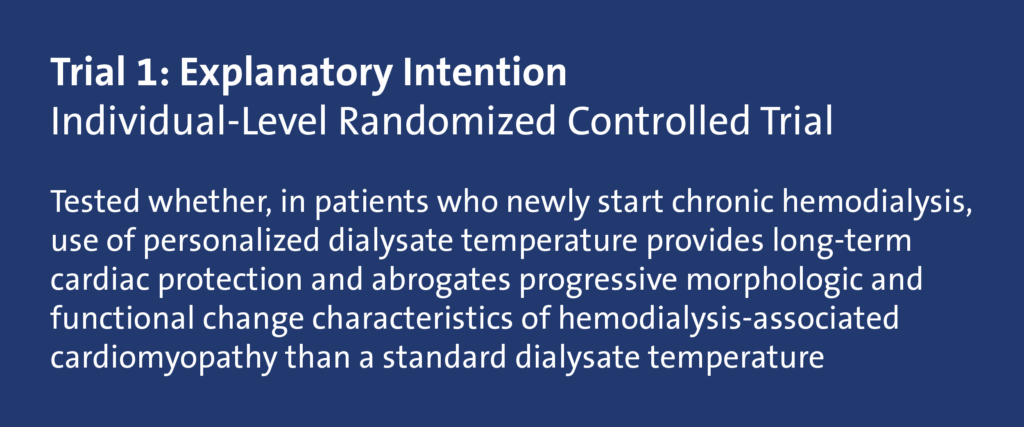
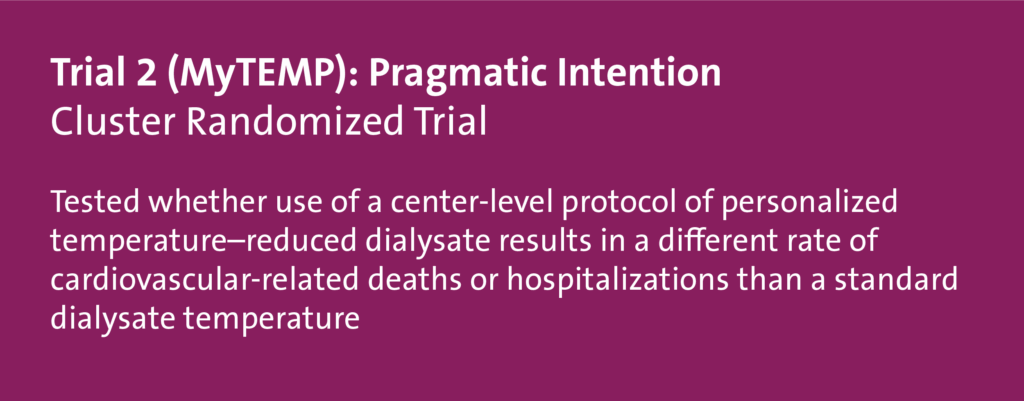
This case study illustrates the design of 2 randomized controlled trials that examined the temperature used in hemodialysis. Using the PRECIS-2 framework, we discuss insights about opportunities and constraints that a renal dialysis setting offers and show how the design of the trials aligned with their intention. Trial 1 was more explanatory in intention, to test a hypothesis about a mechanism of action: that personalizing dialysate temperature would reduce adverse changes in cardiac morphology and function compared with not personalizing the dialysate temperature (Odudu et al 2015). Trial 2 (the MyTEMP trial) was more pragmatic in intention, to help choose between 2 treatment policies by answering the question of whether patients in dialysis centres that personalized dialysate temperature would be better off in terms of cardiovascular death or hospitalization than patients in centers that maintained fixed temperatures (MyTEMP Writing Committee 2022).
We begin with some background on the 2 trials and the PRECIS-2 domains that will guide the step-by-step considerations for situating the trials on the pragmatic-explanatory continuum.
Trial 1 Characteristics (Shaded Blue)
- Personalized dialysis temperature compared with 37° C (98.6° F)
- Unit of randomization: individual patient
- Patients in Nottingham, United Kingdom, enrolled from September 2009 through January 2013
- 1 year of follow-up
- 73 patients would have approximately 11,000 hemodialysis sessions during the trial
- Individual-level consent
- Trial-specific data collection
- Primary outcome: change in the resting ejection fraction measured by cardiac magnetic resonance imaging (MRI) at 12 months compared with baseline
- Cardiac structure, function, and aortic distensibility assessed by cardiac MRI
Trial 2 (MyTEMP) Characteristics (Shaded Red)
- Personalized dialysis temperature compared with 36.5° C (97.7° F)
- Unit of randomization: centers in Ontario followed from April 2017 to March 2021
- Maximum 4 years of follow-up
- 84 centers, 15,413 patients (approximately 6000 entered at start of the trial, approximately 9400 entered during the trial)
- Approximately 4 million hemodialysis sessions during the trial
- Altered consent by patient notification via poster and newsletter, allowing opt-out by patients or providers
- Baseline and follow-up data from large administrative databases
- Primary outcome: a composite of cardiac death or hospital admission with myocardial infarction, stroke, or congestive heart failure
Evaluating the Trials Using PRECIS-2
For study teams, the broad steps of evaluating a trial using the PRECIS-2 wheel include:
- Defining the trial’s intention
- Aligning the design to the intention
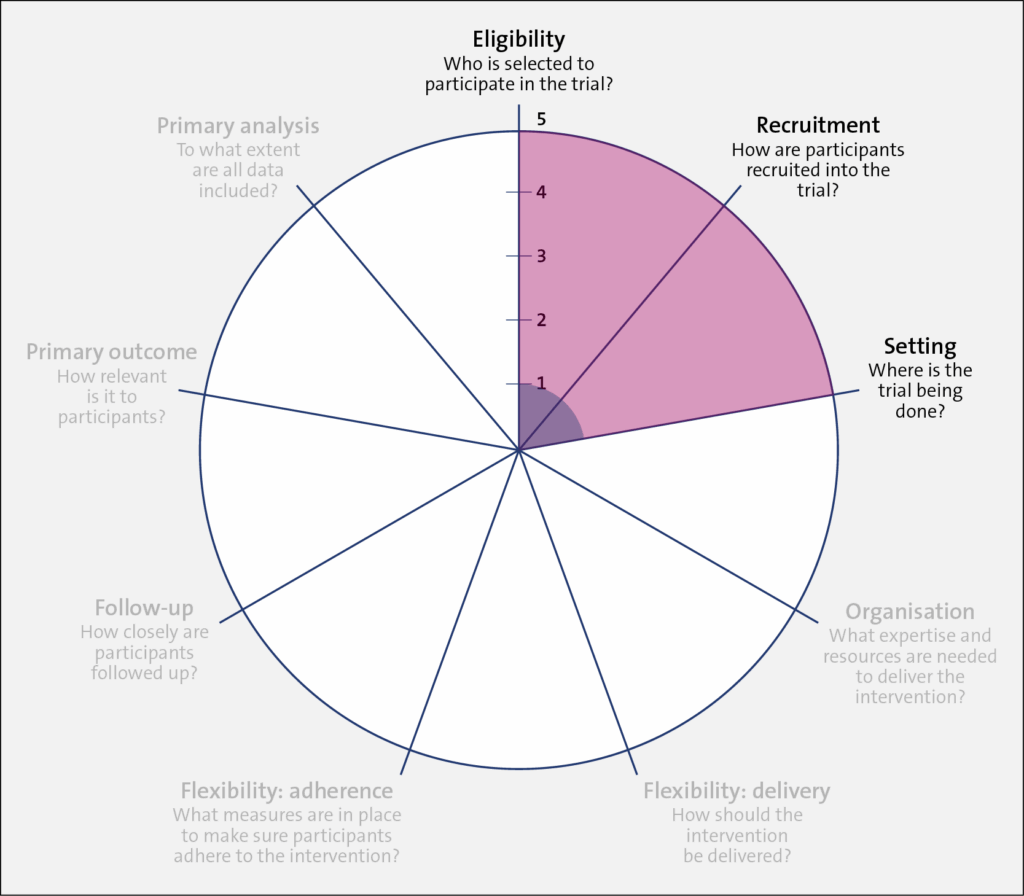
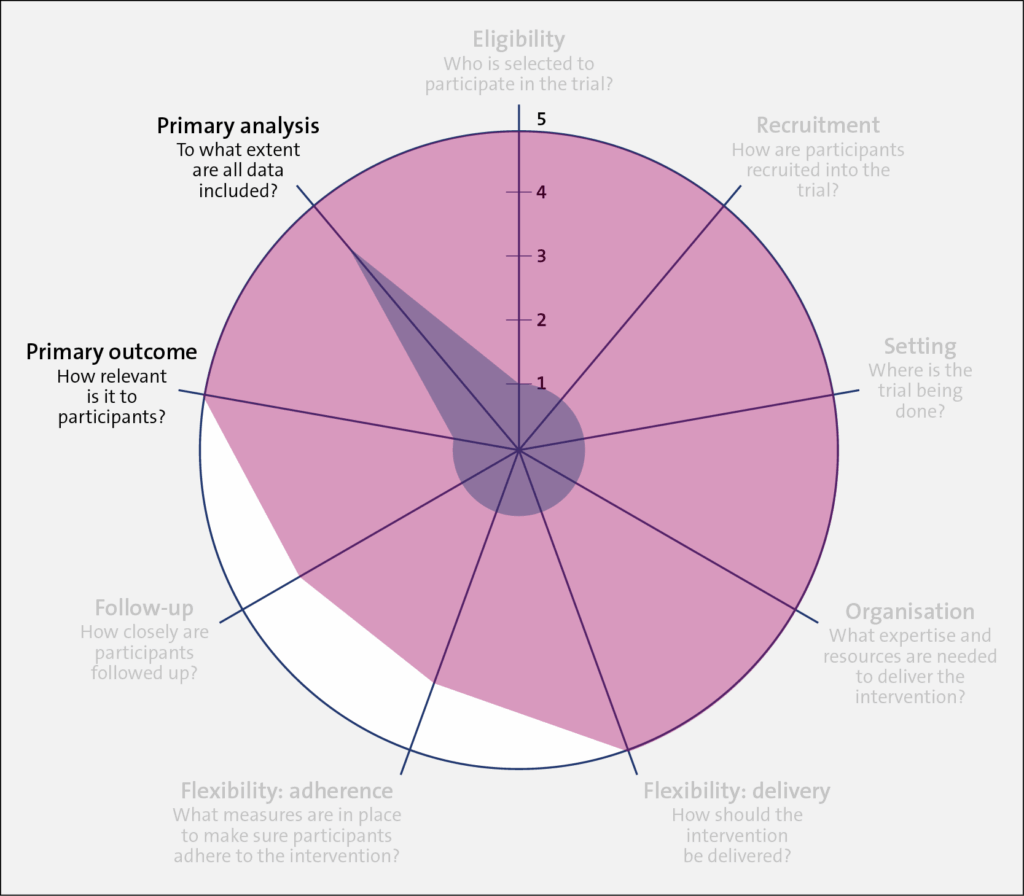
- Identifying the trial’s location on the explanatory-pragmatic continuum (from 1 to 5) for each of the 9 domains (the spokes of the wheel)
Once the intention of the trial is set (pragmatic or explanatory), the designer should align their design choices to their chosen intention across all 9 domains of the PRECIS-2, as outlined in the table below. In this brief discussion, we focus on one of these domains, eligibility, with some mention of the primary outcome.
A very explanatory design approach, with many exclusions and a more physiological outcome (morphology) rather than a patient-centered outcome (mortality), is represented closer to 1 on the PRECIS 2 wheel for each of the domains. Such exclusions may include trial participants who are not adherent to the intervention, who do not respond to treatment, who are at low risk for the primary outcome, and children or older patients. The trial also uses diagnostic tests that are not routine in usual care, to assess both patient eligibility and the primary outcome. On the other hand, a very pragmatic design approach with domains that are set to match as closely as possible those in usual care, that includes almost all patients with the diagnosis, that uses usual diagnostic tests to make the diagnosis, and that chooses outcomes that are directly relevant to patients is represented closer to 5 on the PRECIS-2 wheel.

The Table below summarizes the PRECIS-2 domains and the considerations for each domain.
Table. PRECIS-2 Domains and Considerations
| PRECIS-2 Domain | Considerations |
| Eligibility | To what extent are the participants in the trial like those who would receive this intervention if it was part of usual care? |
| Recruitment | How much extra effort is made to recruit participants over and above what would be used in the usual care setting to engage with patients? |
| Setting | How different are the settings of the trial from the anticipated usual care setting? |
| Organization | How different are the resources, provider expertise, and the care delivery organization in the trial and those available in the anticipated usual care situation? Are extra resources added? |
| Flexibility: delivery | How different is trial flexibility of delivery from flexibility anticipated in usual care? |
| Flexibility: adherence | How different is trial flexibility in monitoring or encouraging adherence from the flexibility anticipated in usual care? |
| Follow-up | How intrusive is measurement and follow-up of participants in the trial vs anticipated follow-up in usual care? |
| Primary outcome | To what extent is the trial’s primary outcome directly relevant to participants? |
| Primary analysis | To what extent are all data included in the analysis of the primary outcome? |
Next, we evaluate the characteristics of both trials and describe the considerations behind each of the 9 PRECIS-2 domains.
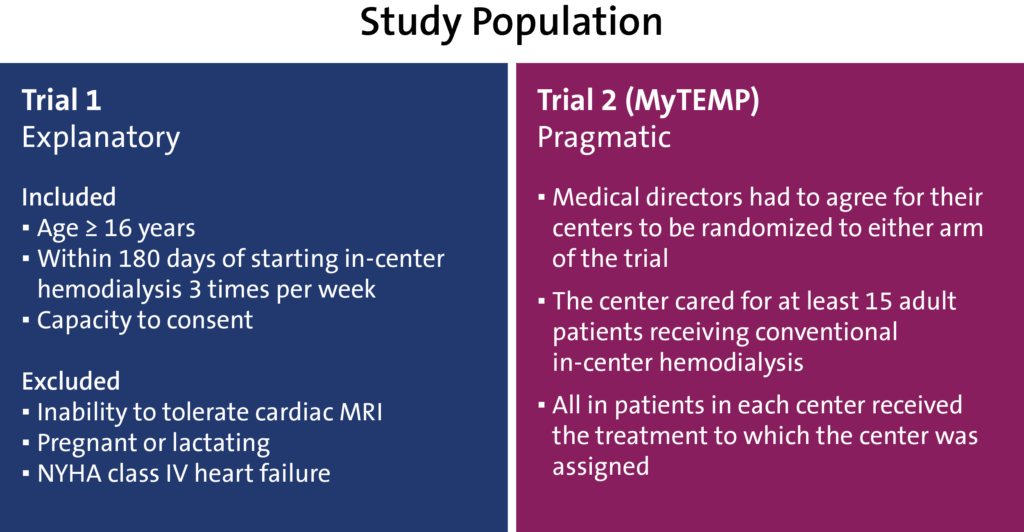
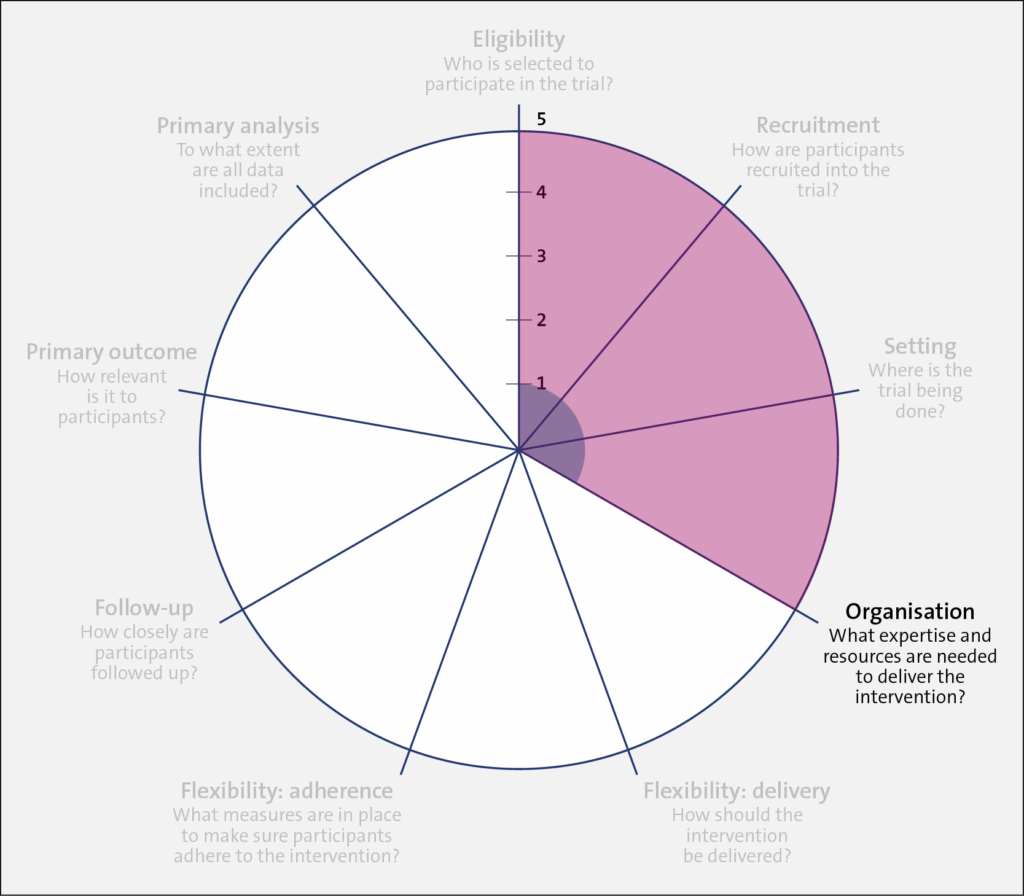
Domains: Eligibility, Recruitment, and Setting
In terms of the trial population, Trial 1 (shaded in blue) was restrictive in its inclusion criteria, having individuals aged 16 years and older who started hemodialysis at the renal clinic setting within the last 180 days and who had the capacity to provide informed consent. In addition, individuals were excluded if they could not tolerate cardiac MRI, were pregnant or lactating, or were classified with New York Heart Association class IV heart failure.
In comparison, Trial 2 (shaded in red) had less restrictive inclusion criteria, which widened its applicability to most usual care providers, patient populations, and settings. For efficiency (that is, ease of trial conduct) and to match the nature of policy on dialysate temperature, which is set by each dialysis center, rather than for individual patients, randomization was at the clinic (or cluster) level. In this design, the medical director of each clinic agreed for their clinic to be randomized to either trial arm, and all patients were part of the trial. A waiver of individual patient consent was sought and granted.
Having a highly pragmatic approach for Trial 2 allowed for the rapid enrollment of clinics and patients (both patients receiving chronic dialysis at the time of randomization and future patients starting dialysis). However, because patients at low and high risk for experiencing the primary outcome were included, a large sample size was required, as nonselectivity reduces the effect size.
Domain: Organization
Trial 1 (shaded in blue) scored low on the PRECIS-2 wheel because the intervention required a specific type of thermometer, trained research staff, a cardiac MRI, and a dialysis machine with the ability to change the dialysis temperature in increments of 0.1 degrees. In comparison, Trial 2 (shaded in red) scored high on the PRECIS-2 wheel because it required no specific expertise or equipment to implement the assigned treatment protocol.
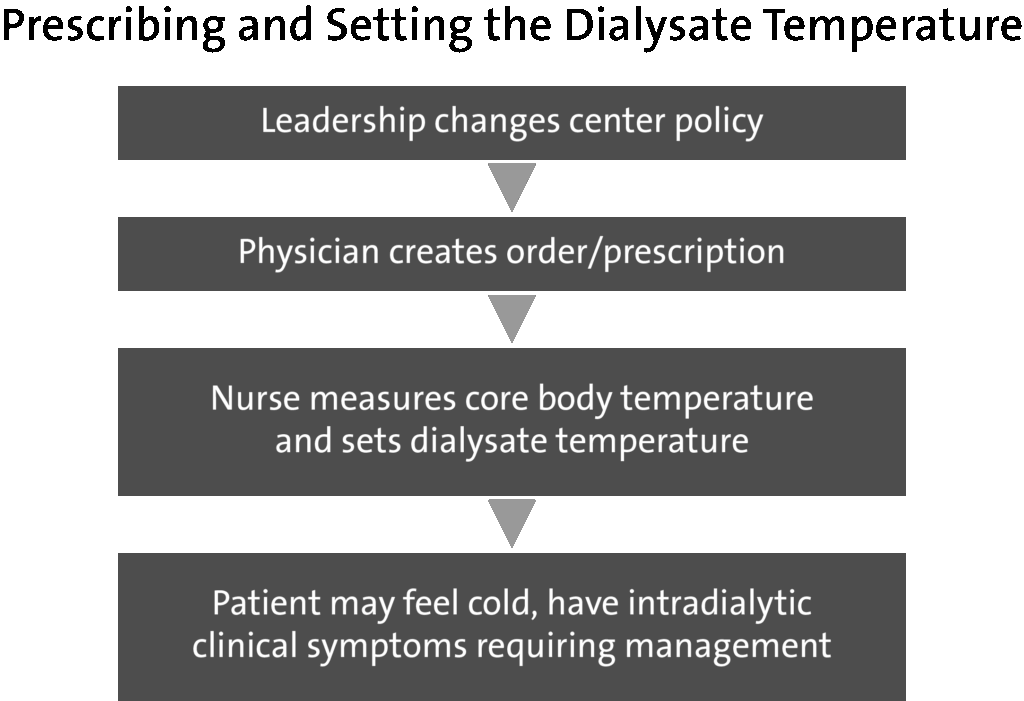
However, because the Trial 2 protocol became the new clinic policy, there was a need to clearly prescribe and set the dialysate temperature. Also, complex roles and social influences on the process of using a personalized dialysate temperature needed to be assessed.
The flowchart below shows the process of who needed to do what differently, the interrelationships between different roles, and the resulting outcomes. In Trial 2, the leadership at each dialysis clinic changed the local policy to ensure alignment with the assigned temperature protocol. Physicians ordered the assigned temperature protocol for current patients at one time and as new patients received prescriptions for dialysate temperature. Nurses were then trained on the trial protocol and asked to follow the physician's orders to set the dialysate temperature. Nurses were also asked to report any issues or adverse clinical symptoms related to dialysate temperature to the treating physician, who could adjust the dialysate temperature as they deemed appropriate.
Domain: Flexibility: Delivery
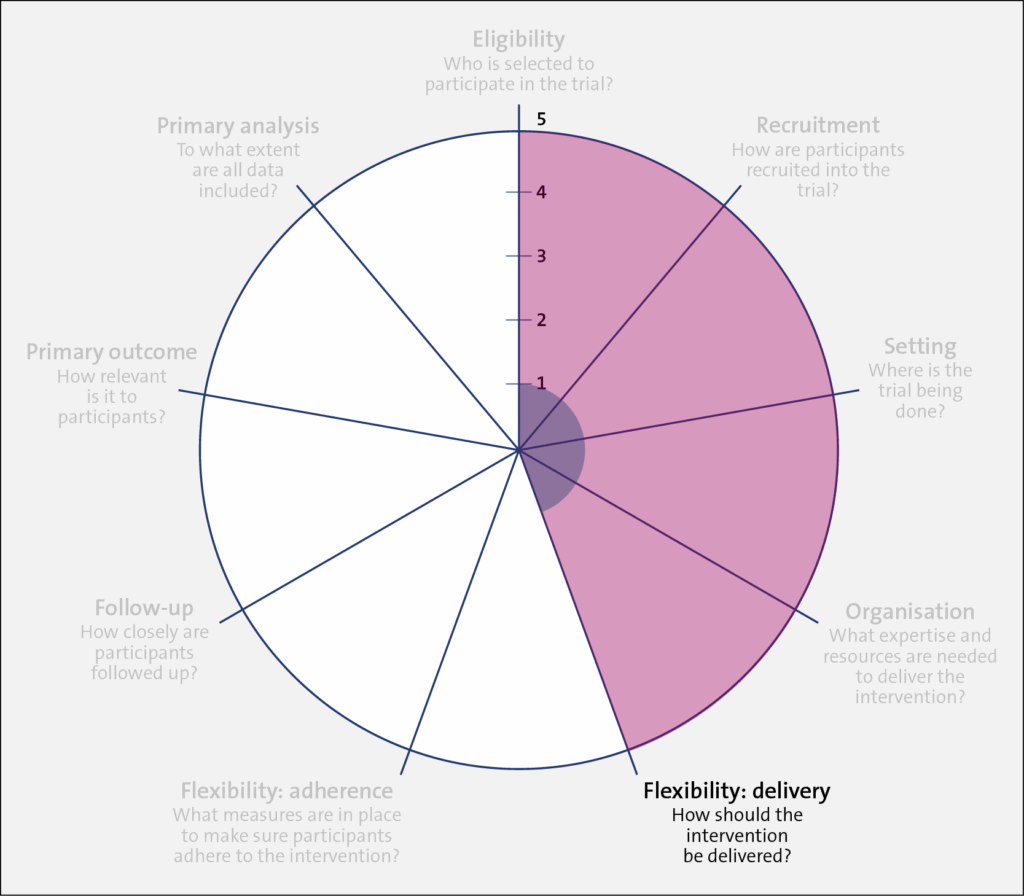
Trial 1 (shaded in blue) required specific dialysis machines, research nurses, and specific thermometers to implement the study intervention. In comparison, Trial 2 retained the dialysis machines in use at each included center and allowed the dialysate temperature in the intervention arm to be set in the range of 0.5 to 0.9 degrees below the patient's body temperature. Also, the entire trial—at the clinic level—was implemented by clinicians and nurses rather than researchers. Little local research infrastructure was required in the recruiting clinics to implement the trial due to this flexibility.
In the control arm of Trial 1 (shaded in red), the dialysate temperature was set to 37° C. In Trial 2, clinics were instructed to set the dialysate temperature to at least 36.5° C, unless the patient or their nephrologist preferred a different temperature.
Domains: Flexibility: Adherence and Follow-up
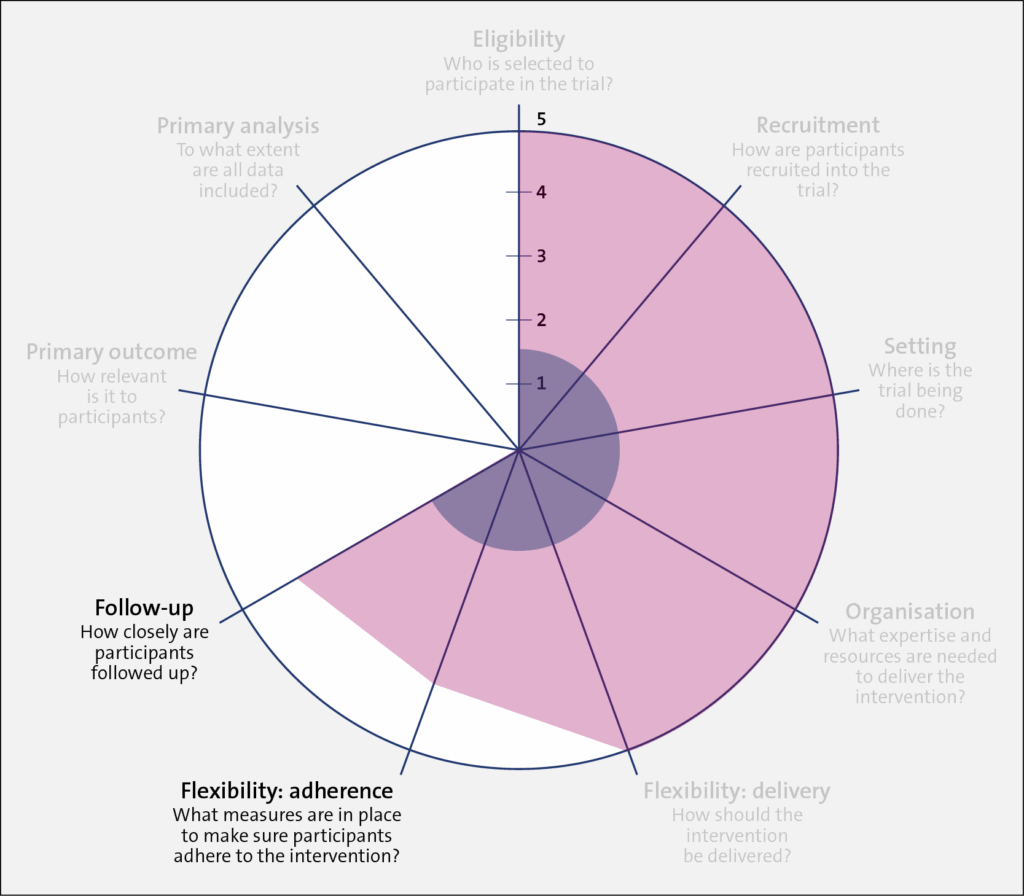
As discussed above, Trial 1 (shaded in blue) employed research staff who closely followed patients for the trial duration. There were regular checkups and feedback sessions between the research staff and participants. In comparison, research staff in Trial 2 (shaded in red) had no contact with participants. However, each month, the clinics were asked to randomly select 15 patients and record the dialysate temperature used for a single session. This allowed the study team to estimate the proportion of patients who were “adhering” to the clinic protocol. It should be noted that the level of adherence for Trial 1 was measured at the participant level, whereas adherence in Trial 2 was measured at the dialysis center. level.
Domains: Primary Outcome and Primary Analysis
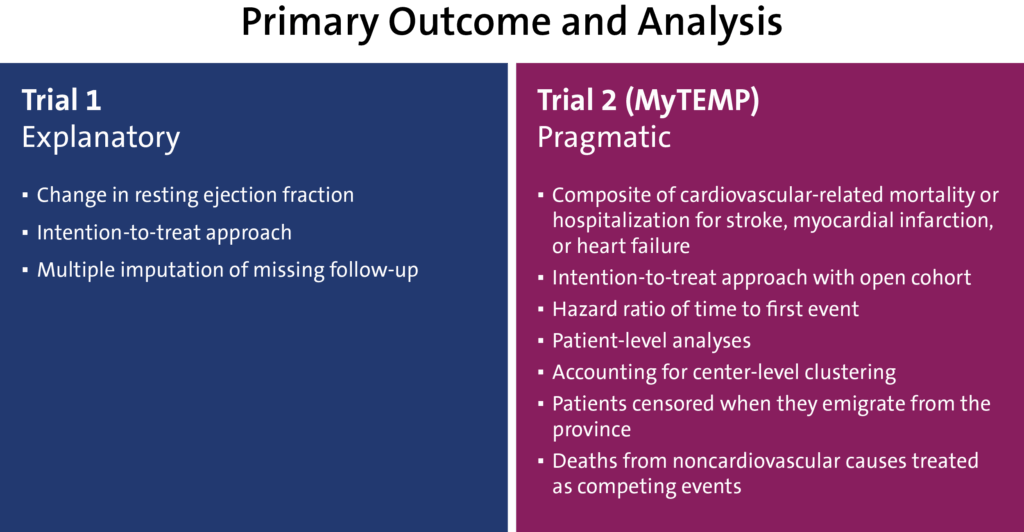
Trial 1 (shaded in blue) had a low PRECIS-2 value (1) for the primary outcome because it tested a change in the resting ejection fraction, which is a surrogate outcome. While important, a change in resting ejection fraction is less relevant to patients. In contrast, for Trial 2, the outcome was cardiovascular-related death or hospital admission for adverse cardiac events, which is of greater relevance to patients and their healthcare providers (PRECIS-2 value 5).
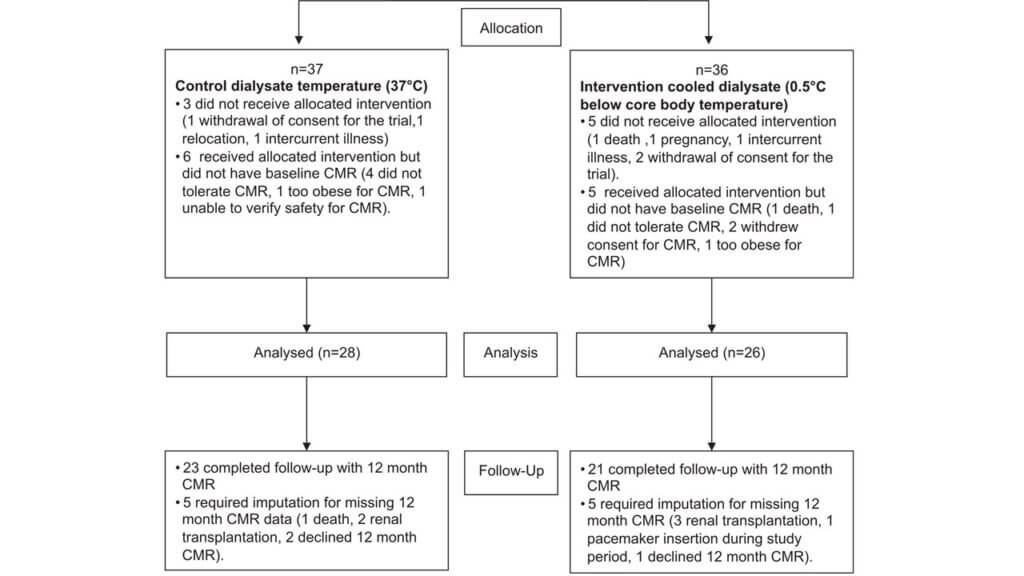
For the analysis domain, Trial 1 used an intention-to-treat approach, which is a highly pragmatic approach. However, nearly 40% of the outcome data was missing due to dropouts or loss to follow-up. From the 73 patients randomized, 37 participants were assigned to the control condition and 36 to the intervention. Of those participants, 28 and 26 were analyzed in the control and intervention arms, respectively. Among those analyzed, data for 5 participants in each arm required multiple imputations for missing outcome data at the 12-month follow-up period.
In contrast, Trial 2 (shaded in red) also used an intention-to-treat approach, but loss to follow-up was expected to be minimal because that typically occurs when study participants leave the (Canadian) province. For example, in Ontario, less than 0.5% the population emigrates from the province each year.
Summary
Pragmatic trials embedded in routine healthcare delivery are increasingly playing a vital role in filling the large gaps in knowledge about caring for patients on hemodialysis. Several fundamental questions in this healthcare setting appear to be particularly suited to pragmatic approaches to trial design. We used Trial 2, the MyTEMP trial, to illustrate a more pragmatic intention, where the authors wanted to test whether the use of a clinic-level protocol of personalized temperature-reduced dialysate results in a different rate of cardiovascular-related deaths or hospitalizations than a standard temperature dialysate. We find it much easier to draw inferences that can be applied to usual care from Trial 2 than we would from Trial 1. The MyTEMP trial was intentionally designed to be highly pragmatic and flexible, which was made possible by:
- Frequent and predictable patient encounters
- Highly granular and uniform electronic data collection in routine care
- Delivery of care by a small number of provider organizations
There is tremendous interest, both nationally and globally, in increasing the momentum for conducting pragmatic trials. Funders of research, including industry sponsors, are increasingly embracing this approach to reduce costs and generate findings that are rapidly translatable to practice.
SECTIONS
Resources
Promoting Both Internal and External Validity: Designing the Trial to Match Its Intention
NIH Pragmatic Trials Collaboratory; August 11, 2021

Pragmatic and Explanatory Attitudes to RCTs: Using the PRECIS-2 Tool to Describe the Design of the MyTEMP Trial; Rethinking Clinical Trials Grand Rounds; November 13, 2020
REFERENCES
MyTEMP writing committee. 2022. Personalised cooler dialysate for patients receiving maintenance haemodialysis (MyTEMP): a pragmatic, cluster-randomised trial. Lancet. 400(10364):1693-1703. doi: 10.1016/S0140-6736(22)01805-0. PMID: 36343653.
Odudu A, Eldehni MT, McCann GP, McIntyre CW. 2015. Randomized controlled trial of individualized dialysate cooling for cardiac protection in hemodialysis patients. Clin J Am Soc Nephrol. 10(8):1408-1417. doi:10.2215/cjn.00200115. PMID: 25964310.
ACKNOWLEDGMENTS
Liz Wing of the NIH Pragmatic Trials Collaboratory Coordinating Center was a contributing editor of a previous version of this chapter.