


Dissemination Approaches for Different Audiences
Section 2
Reporting to the Scientific Community
The settings and methods of pragmatic clinical trials embedded in healthcare systems introduce challenges beyond those faced in traditional explanatory trials. Pragmatic trials also offer opportunities for faster dissemination of results. Moreover, innovations in the design and conduct of pragmatic trials, challenges associated with implementation and sustainment, and the varied interests and perspectives of research partners in pragmatic trials offer a range of opportunities for researchers to publish their work.
Special Considerations for Pragmatic Trials
Because their study interventions are embedded within healthcare settings, such as clinics, hospital units, or healthcare systems, pragmatic clinical trials raise special considerations for authors to support full and transparent reporting. Good reporting allows decision-makers to judge the applicability of the trial results to their own conditions and environments. Full reporting also serves as a foundation for authors as they develop their primary journal publication.
Depending on the particulars of the trial’s design, authors might need to report about:
- How data from electronic health records (EHRs) were used in the research
- Who the research partners were and how they were engaged to participate in the design, conduct, or dissemination of the study
- How unanticipated changes in the study were adjusted for or accommodated
- Whether the trial needed alternate approaches to the informed consent process or other human subjects protections
These considerations are introduced below. More reporting information and guidance for authors is provided in the NIH Collaboratory’s PCT Reporting Template. Moreover, the EQUATOR Network (Enhancing the Quality and Transparency of Health Research) provides a list of reporting guidelines, including guidelines for quality improvement initiatives, explanatory trials, and pragmatic trials. The Table provides links to selected guidelines relevant to pragmatic trials.
Table. Selected Reporting Guidelines Relevant to Pragmatic Clinical Trials
| Reporting Guideline | Name | Study Type |
| SQuIRE 2.0 | Standards for Quality Improvement Reporting Excellence: international writing guidelines for quality improvement publications | Quality improvement |
| CONSORT | Consolidated Standards of Reporting Trials | Randomized trials |
| CONSORT Pragmatic Trial Extension | Improving the Reporting of Pragmatic Trials: An Extension of the CONSORT Statement | Pragmatic trials |
| CONSORT Cluster Trial Extension | Consort 2010 statement: extension to cluster randomised trials | Cluster randomized trials |
| TRIPOD-Cluster Checklist | Transparent Reporting of Multivariable Prediction Models for Individual Prognosis or Diagnosis Developed or Validated Using Clustered Data | Cluster randomized trials |
Secondary Uses of EHR Data
If data for the trial were obtained from a clinical or billing database instead of a data source created primarily for research, good reporting will include such elements as the steps used in gaining permission to use the data, how the population of interest was identified (such as development of phenotypes and use of ICD-10 codes), how data from different sources were linked, how data quality was assessed, the process for data management during the study, the plan for archiving or sharing the data after the study, and any IRB or privacy board review. If the trial employed a research network for querying data (for example, a distributed research network, Clinical and Translational Science Awards [CTSA] program network, or PCORnet partner network), then the network should be described in sufficient detail. Reporting should also address the identifiability of any data, as well as when linking datasets were deidentified. At the end of a study, destruction of data is also a possibility.
Accommodating or Adjusting to Unanticipated Changes in the Study Arms
As trials evolve, changes may occur in the care provided in the intervention or control arms that could affect the conduct or analysis of the study. For example, some components of the intervention may be introduced into usual care at some control sites or clusters. Contamination can occur for various reasons: unintentional spillover of intervention effects, introduction of other healthcare initiatives that focus on the same problem, or changes in leadership, sites, or healthcare delivery system technologies. Authors should describe how they adjusted to such changes, especially if the changes affected the statistical analysis of the trial data.
Learn more in the Unanticipated Changes section of the Analysis Plan chapter of the Living Textbook.
Human Subjects Protection
Authors should describe how approval by an ethics committee or institutional review board (IRB) was obtained or if the IRB determined that the study was exempt from the regulations, and whether HIPAA review was completed by the IRB or a privacy board. Include details such as the type of informed consent (written, oral, information sheet accompanying the consent or waiver of consent), the mode (electronic, mail, in-person). Explain whether a waiver of informed consent was granted for the trial. If applicable, describe the existence of a data monitoring committee. For cluster randomized trials, indicate whether permission was obtained from cluster representatives, individual cluster members, or both. Describe whether consent was obtained before or after randomization.
Faster Dissemination: Preprints and Public Access
The use of preprint servers has grown rapidly as a strategy for accelerating dissemination of research findings. The International Committee of Medical Journal Editors (ICMJE) defines a preprint as “a complete manuscript posted by authors to a preprint server before undergoing peer review and formal publication in a scientific journal.”
By 2020, most of the top-ranked clinical journals allowed preprints and did not consider them to constitute prior publication (Massey et al 2020). The 2 most popular preprint servers in the biomedical sciences—bioRxiv and medRxiv—now post thousands of preprints every month. Since 2013, bioRxiv has posted more than 268,000 preprints from more than 970,000 authors. Since its launch in 2019, medRxiv has posted 64,000 preprints by more than 380,000 authors (Naddaf 2025). Much of the early growth of medRxiv was driven by submissions related to COVID-19 (Krumholz et al 2020). Both repositories recently came under the management of openRxiv, a nonprofit organization launched in 2025 for this purpose (Naddaf 2025).
With the proliferation of preprints, the ICMJE updated its recommendations in 2021 for the reporting of biomedical research to include detailed guidance on the use of preprints. The guidance describes 6 features authors should consider when selecting a preprint archive:
- Identifies preprints as not being peer reviewed
- Requires authors to disclose conflicts of interest
- Requires authors to identify funding sources
- Allows users to report concerns about posted preprints
- Posts withdrawal notices and maintains metadata for withdrawn preprints
- Indicates when a preprint article has been published in a peer-reviewed journal
The ICMJE recommendations also offer standards for citing preprints and discuss the importance of transparency in reporting on the use of preprints by both authors and journals.
In 2023, the National Library of Medicine (NLM) launched phase 2 of its NIH Preprint Pilot. In this project, the NLM makes preprints available in PubMed if the preprint resulted from research funded by the NIH and was posted in 2023 or later. Eligible preprint servers include bioRxiv, medRxiv, arXiv, and Research Square.
The growing use of preprints is part of a broader expansion of public access to research findings. The NIH continues to update its NIH Public Access Policy. Since 2008, this policy has required authors to deposit manuscripts reporting NIH-funded research into the PubMed Central repository upon acceptance for publication. The 2024 revision of the policy removed the ability for publishers to set an embargo period for the availability of these manuscripts. As a result, manuscripts reporting NIH-funded work and accepted for publication on or after July 1, 2025, must be deposited in PubMed Central upon acceptance for publication and be made available without embargo at the time of publication.
Other Publication Opportunities
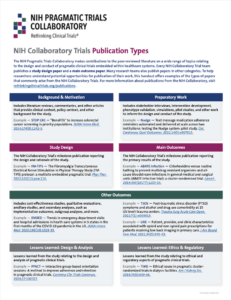
NIH Collaboratory Trial teams publish, at a minimum, a study design paper and a main outcome paper (see Data and Resource Sharing). Many research teams also publish papers of other types. To help researchers understand potential opportunities for publication of their work, the program’s Coordinating Center created the Publication Types handout to offer examples of the types of papers that commonly arise from the NIH Collaboratory Trials. For more information about publications from the NIH Collaboratory, see the program’s Publications webpage.
SECTIONS
Resources
Is It Time to Embrace Preprints? A Conversation About the First 18 Months of medRxiv
NIH Pragmatic Trials Collaboratory PCT Grand Rounds; January 22, 2021
PCT Reporting Template
A template to assist authors with transparent reporting of the primary results of pragmatic clinical trials
NIH Collaboratory Trials Publication Types
A reference to help the NIH Collaboratory Trial teams understand potential opportunities for publication
REFERENCES
Krumholz HM, Bloom T, Sever R, Rawlinson C, Inglis JR, Ross JS. 2020. Submissions and downloads of preprints in the first year of medRxiv. JAMA. 324(18):1903-1905. doi: 10.1001/jama.2020.17529. PMID: 33170232.
Massey DS, Opare MA, Wallach JD, Ross JS, Krumholz HM. 2020. Assessment of preprint policies of top-ranked clinical journals. JAMA Netw Open. 3(7):e2011127. doi: 10.1001/jamanetworkopen.2020.11127. PMID: 32697320.
Naddaf M. 2025. Preprint sites bioRxiv and medRxiv launch new era of independence. Nature. Mar 11. doi: 10.1038/d41586-025-00762-4. Epub ahead of print. PMID: 40069451.
ACKNOWLEDGMENTS
Karen Staman, Gina Uhlenbrauck, and Liz Wing of the NIH Pragmatic Trials Collaboratory Coordinating Center served as contributing editors for previous versions of this chapter.